|
http://dx.doi.org/10.4321/S2254-28842019000100006
Abstract Objective: To investigate the relationship between satisfaction with life in general, sense of humor, and anxiety, depression and stress with subjective happiness in chronic kidney disease patients undergoing hemodialysis. Material and Methods: A cross-sectional and correlational study was developed in two units of the Diaverum dialysis clinic and one hospital unit, with 183 chronic kidney disease patients undergoing hemodialysis. An instrument was used to characterize the sociodemographic and clinical profile of the sample (age, gender, nationality, education, occupation, marital status, dialysis sessions length, presence of hypertension and diabetes): the subjective happiness scale; the satisfaction with life in general; depression, anxiety and stress scale 21; and multidimensional sense of humor scale. Inferential procedures included Spearman correlation coefficients, and multiple linear regression adjusting to age, marital status, professional activity and diabetes. Results: Subjective Happiness was positively correlated with satisfaction with life in general, and the three dimensions of Sense of Humor. Nevertheless, subjective happiness was negatively correlated with stress / anxiety and depression. Satisfaction with life in general, humor production and social use of humor, and attitude towards humor had a positive relationship with subjective happiness. However, depression had a negative relationship with subjective happiness. Conclusions: Higher levels of subjective happiness were associated with higher levels of satisfaction with life in general, and sense of humor, however they were also associated with lower levels of depression in patients undergoing hemodialysis. KEYWORDS: renal dialysis; happiness; wit and humor as topic; depression.
Introduction Hemodialysis (HD) is the main treatment for patients in end-stage renal disease, however, it presents a high risk for adverse patient outcomes1. HD affects the life of Chronic kidney disease (CKD) patients and it can have negative effects on general health and well-being including mental, social, physical, emotional, spiritual, and subjective aspects. Furthermore, it can have a negative influence on physical performance, mental status, and social relationships2. Anxiety, depression and stress are frequent conditions in CKD patients, essentially during the transition from the pre-dialysis period to renal replacement therapy. Nevertheless, it tends to decrease after beginning dialysis3. The World Health Organization (WHO) points out that subjective wellbeing is considered within the research community as an indicator of Quality of Life evaluation4. The subjective wellbeing is characterized by emotional responses, satisfaction domains, and the judgment about global satisfaction with life. The subjective wellbeing components are pleasant affect (e.g. joy, contentment, pride, affection, and happiness), unpleasant affect (e.g. guilt and shame, anxiety and worry, anger, stress, and depression), life satisfaction (e.g. desire to change, satisfaction with current life, past, and future), and a satisfaction domain (e.g. work, family, leisure, health, finances, and self)5. In the CKD patients the subjective wellbeing (measured by personal wellbeing index) is positively related with subjective happiness, positive affect, and quality of life and is negatively associated with negative affect. Subjective happiness, negative affect, and the physical component of quality of life are associated to the subjective wellbeing6. Moreover, higher levels of happiness are associated with higher levels of satisfaction with life in general (personal wellbeing index)7, and also with higher levels of sense of humor8. This study intends to disclose if CKD patients’ subjective well-being, sense of humor, and anxiety, depression and stress are significant predictors of their subjective happiness, further influencing patients’ disease management strategies and health status. The objective was to investigate the relationship between subjective well-being, sense of humor, and anxiety, depression and stress with subjective happiness in CKD patients undergoing hemodialysis. Material and Methods Study design
Subjects and setting
Procedures
Various instruments were used to characterize the socio demographic and clinical profile of the sample (age, gender, nationality, education, occupation, marital status, dialysis sessions length, presence of hypertension and diabetes), the subjective happiness scale (SHS)7; the satisfaction with life in general (SWLG) was measured by the Personal Wellbeing Index9; Depression, Anxiety and Stress Scale 21 (DASS – 21)10; and Multidimensional Sense of Humor Scale (MSHS)8. Outcomes measurement
The MSHS structure was globally consistent with studies conducted in other samples, presenting satisfactory internal consistency values. It is considered a valid instrument for characterizing an individual’s “state of humor” and to describe its different dimensions. The Portuguese version of MSHS showed a structure with three factors, “Humor Production and Social Use of Humor”, “Adaptive Humor and Appreciation Humor” and “Attitude Towards Humor”, with Cronbach’s a values of 0.93, 0.90 and 0.83 respectively8. Ethical approval
Data analysis
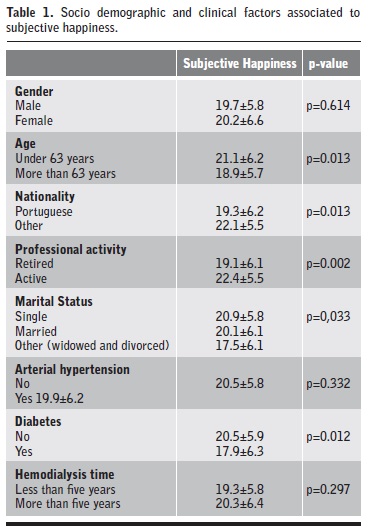
Results The sample consisted of 183 patients diagnosed with CKD, with an average age of 59.17 (±14.64) years, mostly men (59.6%). The nationality of the patients was distributed as follows: most patients are Portuguese (78.7%), followed by Cape Verdean (13.7%), Sao Tomean (3.3%), Angolan (2.2%), Guinean (1.6%), and Bulgarian (0.5%). Concerning literacy level, 3.3% were illiterate, 41.1% had the 4th grade, 18.9% the 6th grade, 15% the 9th grade, 12.2% the 12th grade and 9.4% university education. In this sample 28% of the patients were single, 53.8% married, 11.5% widowed and 6.6% divorced. Concerning occupation, 76% were retired while 24% had a regular job. Regarding health data, patients underwent hemodialysis for 70.09 (±54.2) months, 61.9% had high blood pressure and 25.8% diabetes. CKD patients under 63 years of age had higher levels of subjective happiness (p=0.013) than older patients. Portuguese CKD patients had the lowest score for subjective happiness (p=0.013), compared with the remaining population (Cape Verdean; São Toméan; Angolan, Guinean and Bulgarian). Retired patients had lower levels of subjective happiness (p=0.002) than those who have regular jobs. Widowed and divorced patients had lower levels of subjective happiness (p=0.033) in comparison to married and single patients (Bonferroni correction). Finally, CKD patients with diabetes had a lower level of subjective happiness (p=0.012). Table 1 shows both socio demographic and clinical factors related with CKD, that are associated with subjective happiness. | |
| |
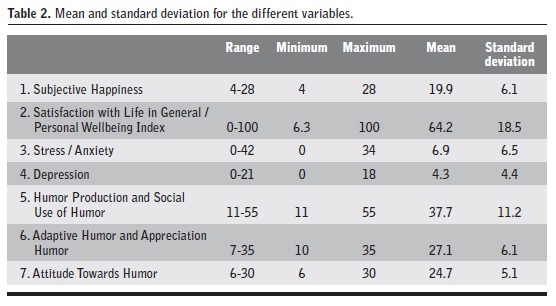
Mean score of subjective happiness was 19.9 (±6.1), satisfaction with life in general/personal wellbeing index has a mean score of 64.2% (±18.5%). Mean scores for the other variables are as following: stress/anxiety 6.9 (±6.5); depression 4.3 (±4.4); humor production and social use of humor 37.7 (±11.2); adaptive humor and appreciation humor 27.1 (±6.1) and attitude towards humor with 24.7 (±5.1) (Table 2). | |
| |
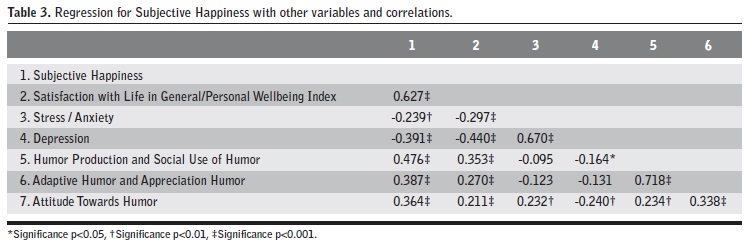
Table 3 shows that the subjective happiness was positively correlated with professional activity (?=0.256, p<0.01); satisfaction with life in general/personal wellbeing index (?=0.627, p<0.001), humor production and social use of humor (?=0.476, p<0.001); adaptive humor and appreciation humor (?=0.387, p<0.001); and attitude towards humor (?=0.364, p<0.001). However, it presented a low negative correlation with stress/anxiety (?=-0.239, p<0.01) and depression (?=-0.391, p<0.001). Higher scores on subjective happiness were associated with higher levels of satisfaction with life in general/personal wellbeing index, humor production and social use of humor, adaptive humor and appreciation humor and attitude towards humor, though lower levels of subjective happiness were associated with higher levels of stress/anxiety and depression. | |
| |
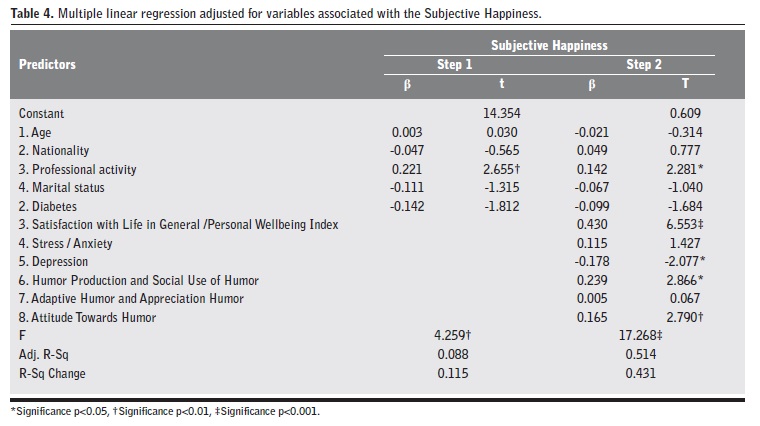
Professional activity was negatively correlated with depression (?=-0.222, p<0.001), satisfaction with life in general/personal wellbeing index was positively correlated with humor production and social use of humor (?=0.353, p<0.001); adaptive humor and appreciation humor (?=0.270, p<0.001) and attitude towards humor (?=0.211, p<0.001). Nevertheless, it presented a negative correlation with stress/anxiety (?=-0.297, p<0.001) and depression (?=-0.440, p<0.001). Higher scores on satisfaction with life in general/personal wellbeing index were associated with higher levels of humor production and social use of humor, adaptive humor and appreciation humor, and attitude towards humor, and lower levels of stress/anxiety and depression. Stress/anxiety showed a significant positive correlation with depression (?=0.670, p<0.001) and attitude towards humor (?=0.232, p<0.01). Depression was negatively correlated with humor production, with social use of humor (?=-0.164, p<0.05) and with attitude towards humor (?=-0.240, p<0.01). When depression values increased, humor production and social use of humor and attitude towards humor values decreased. Humor production and social use of humor showed a significant positive correlation with adaptive humor and humor appreciation (?=0.718, p<0.001); and attitude towards humor (?=0.234, p<0.001). Lastly, adaptive humor and humor appreciation were positively correlated with attitude towards humor (?=0.338, p<0.001). The model with professional activity, explains 8% of the subjective happiness variance. This control variable is the one that most contributes to the explanation of subjective happiness (?R2=0.115, p<0.01). In the second step, the adjusted R2 for the model was 51.4% for professional activity, satisfaction with life in general/personal wellbeing index, stress/anxiety, depression, humor production and social use of humor, and attitude towards humor, being these the variables that best explain subjective happiness. The resulting R2 were statistically significant at the p<0.00 and p<0.05 levels. Professional activity, satisfaction with life in general/personal wellbeing index, humor production and social use of humor, and attitude towards humor had a positive effect on subjective happiness (respectively, ß=0.142, p<0.05; ß=0.430, p<0.001; ß=0.239, p<0.05; ß=0.165, p<0.01). Nevertheless, depression had a negative effect on subjective happiness (ß=-0.178, p<0.05).These variables are the ones contributing the most to the explanation of subjective happiness (?R2=0.431, p<0.001). Discussion Our study was aimed at examining the relationship between subjective happiness and satisfaction with life in general/personal wellbeing index, stress/anxiety and depression, sense of humor and socio-demographic characteristics, as well as, verifying the relationship between these variables and subjective happiness. The findings are aligned with the literature on the effects of HD on CKD patients’ life, and on the psychological stressors that may decrease wellbeing and quality of life, therefore contributing to less positive clinical outcomes11. The highest levels of happiness were found in younger CKD patients with regular employment, married or single, non-Portuguese nationality and without diabetes. These results also corroborate the findings of another study carried out in patients undergoing hemodialysis, namely, standard of living and satisfaction with life achievements carried higher importance in subjective wellbeing12. Such results can also be partly explained by the aging process. Older people patients on hemodialysis have peculiar characteristics, not only because of the greater number of associated comorbidities, but because the aging process itself entails physical and psychological changes that directly affect quality and life. Other aspects must also be considered as high stress factors during hemodialysis sessions13, such as the vascular access, which includes the cannulation process, bleeding, infection, lack of flow, and the inexperience of the team. Having a job minimizes the impact of the treatment routine, it makes the individual feel useful and socially active, which explains higher levels of personal fulfillment and greater happiness. One study points out that by the end of 2015, approximately 36% of patients undergoing peritoneal dialysis had full-time work, contrasting with 22% of hemodialysis patients14. Despite the impact of treatment on the personal routine, married patients find in their family nuclei an informal but more solid support network, which strengthens their emotional component and eventually their perception of happiness. On the other hand, widowers under hemodialysis experience more hopelessness and had lower level of general health15, probably because they have nobody to share their sorrows, maintaining their feelings on the burden of disease16. These patients consequently have greater difficulty in finding adaptive strategies that allow maintaining or increasing their levels of happiness. Concerning nationality, the non-Portuguese patients of our sample are predominantly African. The higher levels of happiness found in this population may be explained by cultural issues, as these individuals live in larger family and social networks with expanded support. This idea is supported, in part, by a study that observed a level of low contentment, and medium to high levels of hedonic affection in a group of black Africans17. Happiness can influence socioeconomic phenomena such as consumption activities, behavior at work, investment behavior and political behavior, presenting itself as a determining factor in person´s quality of life18. In the same way, happiness was associated with higher levels of satisfaction with life in general, humor production and social use of humor, adaptive humor and appreciation humor and attitude towards humor. Though lower levels of subjective happiness were associated with higher levels of stress/anxiety and depression. The psychological disorders are the most common problems in patients undergoing dialysis, such as depression and anxiety. Hemodialysis is considered a long-term treatment and has significant side effects on physical and mental well-being19. Stress is a common reaction of patients with CKD undergoing HD which appears as a way to deal with the anxiety associated with the threat of the disease. Since they are constantly alert, they are also more vulnerable and have more difficulty in keeping an emotional state of happiness. Such findings may have important clinical implications for these patients. Untreated mental problems increase mortality, decrease quality of life, and increase the risk of suicide19. Healthcare teams must consider the need for a periodic evaluation of the stressors and their effects on the health and quality of life of the patients, with the consequent development of strategies that offer these individuals interventions that propitiate an improvement in their quality of life. Patients undergoing hemodialysis with higher levels of subjective happiness were found to be associated with higher levels of satisfaction with life in general9. CKD patients with higher levels of sense of humor were associated with higher levels of subjective happiness and satisfaction with life in general8. Professional activity, satisfaction with life in general, humor production and social use of humor, and attitude towards humor had a positive effect on subjective happiness. Thus, depression had a negative effect on subjective happiness. Fordyce’s happiness program was effective in reducing depression and anxiety11,20 and improving life of quality of patients undergoing hemodialysis20. Keeping in mind the limitations and implications for practice of this study, we emphasize the need for further studies on nursing interventions under the promotion of happiness in the most diverse contexts of the practice of care for the person with chronic kidney disease. Its disclosure is imperative. Practical implications for nursing
Such results may also help future interventions related to the emotional wellbeing (subjective happiness) of CKD patients, particularly those aimed at improving nurse training and the identification of nursing diagnosis related to well-being and monitoring the effectiveness of nursing interventions. Nurses with this knowledge could be able to optimize their patients’ health outcomes. Depressive symptoms in CKD patients are associated with decreased wellbeing16 and consequently decreased quality of life21-22. In fact, with our data we can infer that when nurses implement interventions that increase the perception of subjective happiness, they can improve the patients’ well-being and, consequently, their quality of life when patients undergoing hemodialysis however, further research is required. Several authors point out the Fordyce’s happiness program11,20, the integration of laughter yoga23, the simulated laughter programme24 or watching humor movies, according to the patients’ preferences25, as important strategies to increase CKD patients’ happiness. Limitations
From the results found we can conclude about the relationship between subjective well-being, sense of humor, and psychological health with subjective happiness in CKD patients. Satisfaction with life in general/personal wellbeing index, humor production and social use of humor, and attitude towards humor had a positive relationship with subjective happiness. However, depression had a negative relationship with subjective happiness. | |
| |
References 1. Rivara MB, Chen CH, Nair A, Cobb D, Himmelfarb J, Mehrotra R. Indication for dialysis initiation and mortality in patients with chronic kidney failure: a retrospective cohort study. Am J Kidney Dis. 2017;69(1):41-50. 2. Seraji M, Shojaeizadeh D, Rakhshani F. Well-being in Hemodialysis Patients. Iran J Public Health. 2018;47(8):1222-3. 3. Bezerra CI, Silva BC, Elias RM. Decision-making process in the pre-dialysis CKD patients: do anxiety, stress and depression matter? BMC Nephrol. 2018;19(1):98. 4. Weinberg MK, Bennett PN, Cummins RA. Validation of the personal wellbeing index for people with end stage kidney disease. Appl Res Qual Life. 2016;11(4):1227-40. 5. Diener E, Suh EM, Lucas RE, Smith HL. Subjective well-being: Three decades of progress. Psychol Bull. 1999;125(2):276-302. 6. Sousa LM, Antunes AV, Baixinho CR, Severino SS, Marques-Vieira C, José HM. Subjective Wellbeing Assessment in People with Chronic Kidney Disease Undergoing Hemodialysis. In T Rath (Ed.) Chronic Kidney Disease - from Pathophysiology to Clinical Improvements. InTech; 2018:281-93 DOI: 10.5772/intechopen.71194. 7. Sousa LM, Marques-Vieira CM, Severino SS, Pozo-Rosado JL, José HM. Validation of the Subjective Happiness Scale in people with Chronic Kidney Disease. Enferm Global. 2017;16(3):60-70. 8. Sousa LMM, Marques-Vieira CM, Severino S, Pozo-Rosado J, Antunes AV, José HM. Validation of the multidimensional sense of humor scale in people with chronic kidney disease. J Nurs Educ Pract. 2018;8(3):72-9. 9. Sousa LMM, Marques-Vieira CMA, Severino SSP, Pozo Rosado JL, José HM. Validación del Índice de Bien-estar Personal en personas con enfermedad renal crónica. Enferm Nefrol. 2016;19(2):135-41. 10. Sousa LM, Marques-Vieira CM, Severino SS, Correo JL, Gomes JC, José HM. A Depression Anxiety Stress Scale em pessoas com doença renal crónica. Rev Port Enferm Saúde Ment. 2017;17:50-7. 11. Mehrabi Y, Ghazavi Z, Shahgholian N. Effect of fordyce’s happiness program on stress, anxiety, and depression among the patients undergoing hemodialysis. Iran J Nurs Midwifery Res. 2017; 22(3):190-4. 12. Bennett PN, Weinberg MK, Bridgman T, Cummins RA. The happiness and subjective well being of people on haemodialysis. J Ren Care. 2015;41(3):156-61. 13. Casey JR, Hanson CS, Winkelmayer WC, Craig JC, Palmer S, Strippoli GF, et al. Patients’ perspectives on hemodialysis vascular access: a systematic review of qualitative studies. Am J Kidney Dis. 2014;64(6):937-53. 14. Jin DC, Yun SR, Lee SW, Han SW, Kim W, Park J. Current characteristics of dialysis therapy in Korea: 2015 registry data focusing on elderly patients. Kidney Res Clin Pract. 2016;35(4):204-11. 15. Shakya D, Tuladhar J, Poudel S. Burden and Depression among Caregivers of Hemodialysis Patients. Palliat Med Care. 2017;4(1):1-6. 16. Ercan F, Demir S. Hopelessness and Quality of Life Levels in Hemodialysis Patients. Gazi Med J. 2018;29(3):169-174. 17. Brulé G, Veenhoven R. Geography of happiness: configurations of affective and cognitive appraisal of life across nations. Int J Happiness Dev. 2015;2(2):101-17. 18. Sulemana I. Are happier people more willing to make income sacrifices to protect the environment? Soc Indic Res. 2016;127(1):447-67. 19. El Filali A, Bentata Y, Ada N, Oneib B. Depression and anxiety disorders in chronic hemodialysis patients and their quality of life: a cross-sectional study about 106 cases in the northeast of Morocco. Saudi J Kidney Dis Transplant. 2017;28(2):341-8. 20. Tabatabaei MF, Raghibi M. Effect of happiness training in depression, anxiety, and quality of life among hemodialysis patients. J Res Health. 2017;7(4):935-43. 21. Belayev LY, Mor MK, Sevick MA, Shields AM, Rollman BL, Palevsky PM, et al. Longitudinal associations of depressive symptoms and pain with quality of life in patients receiving chronic hemodialysis. Hemodial Int. 2015;19(2):216-24. 22. Ottaviani AC, Betoni LC, Pavarini SC, Gramani Say K, Zazzetta MS, Orlandi FD. Association between anxiety and depression and quality of life of chronic renal patients on hemodialysis. Texto Contexto Enferm. 2016;25(3):e00650015. 23. Bennett PN, Parsons T, Ben-Moshe R, Neal M, Weinberg MK, Gilbert K, et al. Intradialytic Laughter Yoga therapy for haemodialysis patients: a pre-post intervention feasibility study. BMC Complemt Altern Med. 2015;15(1):176. 24. Heo EH, Kim S, Park HJ, Kil SY. The effects of a simulated laughter programme on mood, cortisol levels, and health-related quality of life among haemodialysis patients. Complement Ther Clin Pract. 2016;25:1-7. 25. Sousa LM, Marques-Veira C, Severino SS, Pozo-Rosado JL, José HM. Fatores explicativos da apreciação de filmes cómicos em pessoas com doença renal crónica. Rev Inv Enferm. 2016;S2(15):49-55. Este artículo se distribuye bajo una Licencia Creative Commons Atribución-NoComercial 4.0 Internacional.
| |
|