|
http://dx.doi.org/10.4321/S2254-28842019000300004
Como citar este artículo:
Abstract Objective: To evaluate whether visualization of humor movies during hemodialysis sessions improves subjective well-being and sense of humor, while decreasing stress / anxiety and depression levels, in hemodialysis patients. Material and Method: A pre-test / post-test design study with a non-equivalent control group was carried out in patients with chronic kidney disease undergoing hemodialysis, in two hemodialysis units of Diaverum Clinics. The study included 34 patients in the intervention group and 33 patients in the control group. The intervention consisted in the visualization of humor movies during hemodialysis sessions for ten sessions over a four-week period. The control group watched neutral movies. Data were collected using a sociodemographic and health information questionnaire (age, gender, nationality, education, occupation, marital status, dialysis session length, presence of hypertension and diabetes); the Subjective Happiness Scale; the satisfaction with life in general; the Depression Anxiety Stress Scale 21, and the Multidimensional Sense of Humor Scale. Student t-tests and t-tests for paired samples were performed. The response to change was evaluated using: the percentage of change, ceiling effect and floor effect, effect size, and the standardized response mean. Results: The levels of subjective happiness and sense of humor increased in the intervention group, but there were no significant increases in satisfaction with life in general. Only depression levels decreased significantly in the intervention group. Conclusions: The visualization of humor movies as a nursing intervention improved the levels of subjective happiness and sense of humor, while decreasing the perception of depressive symptoms. KEYWORDS: renal dialysis; happiness; quality of life; depression; wit and humor as topic.
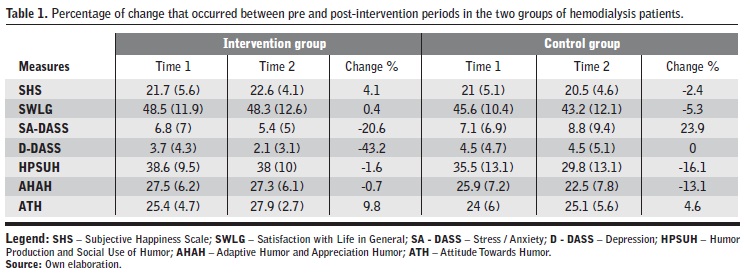
Efecto del uso del humor en el bienestar, depresión y sentido del humor en pacientes en hemodiálisis Resumen Objetivo: Evaluar si la visualización de películas de humor durante las sesiones de hemodiálisis mejora el bienestar subjetivo y el sentido del humor, al tiempo que disminuye los niveles de estrés / ansiedad y depresión, en pacientes con hemodiálisis. Material y Método: Se realizó un estudio pre-post intervención con un grupo de control no equivalente, en pacientes con enfermedad renal crónica en hemodiálisis, en dos unidades de hemodiálisis de Diaverum Clinics. El estudio incluyó a 34 pacientes en el grupo de intervención y 33 pacientes en el grupo de control. La intervención consistió en la visualización de películas de humor durante diez sesiones de hemodiálisis en un período de cuatro semanas. El grupo control vio películas neutrales. Los datos se recogieron mediante un cuestionario de información sociodemográfica y de salud (edad, sexo, nacionalidad, educación, ocupación, estado civil, duración de la sesión de diálisis, presencia de hipertensión y diabetes); la escala subjetiva de felicidad; la escala de satisfacción general con la vida; la escala de depresión, ansiedad y estrés (DASS-21) y la escala multidimensional de sentido del humor. Se emplearon pruebas t-Student y pruebas t para muestras pareadas. La respuesta al cambio se evaluó utilizando: el porcentaje de cambio, el efecto pico y el efecto base, el tamaño del efecto y la media de respuesta estandarizada. Resultados: Los niveles de felicidad subjetiva y de sentido del humor aumentaron en el grupo de intervención, pero no hubo aumento significativo en la satisfacción general con la vida. Solo los niveles de depresión disminuyeron significativamente en el grupo de intervención. Conclusiones: La visión de las películas de humor como una intervención de enfermería mejoró los niveles de felicidad subjetiva y de sentido del humor, al tiempo que disminuyó la percepción de los síntomas depresivos. PALABRAS CLAVE: diálisis renal; felicidad; calidad de vida; depresión; ingenio y humor como tema. Introduction Hemodialysis leads to changes in the lifestyle of both patients and their families, presenting limitations in terms of emotional, economic, social and occupational aspects. It is also observed that the constant exposure to adverse factors inherent to Chronic Kidney Disease (CKD), such as the time spent in the hemodialysis sessions, the constant medical appointments, the laboratory tests, the diet, the expectation of transplantation and the frequent hospital admissions, have contributed to the emergence of psychoaffective diseases1. Patients undergoing hemodialysis suffer several changes in their lives, due to both illness and treatment. It causes anxiety and depressive disorders, emotional state changes2, and it has consequences in the patients’ well-being and quality of life3. These psychological and emotional conditions are influenced by life metamorphosis (what disease and treatment causes in a person’s life), by the various types of pain they experience, and by the way treatment invades the person’s life4. Nevertheless, a study performed in CKD patients verified that the physical component of Quality of Life (QoL) is positively related to dimensions of subjective well-being, namely: subjective happiness, satisfaction with life in general, and positive affect. Furthermore, the mental component of QoL is positively associated with subjective happiness, satisfaction with life in general, positive affect, and negatively related to negative affect5. Subjective happiness, negative affect and the physical component of the QoL, all influence the cognitive dimension of subjective well-being (satisfaction with life in general)4. In this sense, there have been studies that prove the effectiveness of humor intervention such as, laughter yoga6 and the happiness reinforcement program7, in CKD patients during dialysis. Together with the different theoretical approaches, in an attempt to evaluate the effects of humor on health, several methodological approaches are advocated to investigate these effects. The most commonly used approaches include experimental studies and simple correlational studies. In the experimental approach, participants are typically exposed to comedy audios or videos, alone or in small groups and in a controlled environment8. According to the aforementioned, the aim of the study was to evaluate whether the visualization of humor movies during hemodialysis sessions improves subjective well-being and sense of humor, while decreasing stress / anxiety and depression levels, in these patients. The specific objectives were: 1) To determine if watching humor movies during hemodialysis sessions improves subjective well-being in hemodialysis patients, that is, subjective happiness, satisfaction with life in general; 2) To analyze if watching humor movies during hemodialysis sessions decreases stress / anxiety and depression levels in hemodialysis patients; 3) To evaluate if watching humor movies during hemodialysis sessions improves hemodialysis patients’ sense of humor. Material and Methods Study design This is a study with a pre-test / post-test design with a non-equivalent control group, in patients undergoing hemodialysis, in two hemodialysis units of Diaverum, in Lisbon, between May and June 2015. Subjects and setting As inclusion criteria, we defined: above 18 years of age, appreciate humor and motivation to participate in the study. The exclusion criteria were the following: does not appreciate humor, acute psychiatric illness, cognitive deficit and presence of visual impairment or unbalanced hearing loss. From the previous information, data collection related to humor assessment, namely humor appreciation, was verified using a humor evaluation scale9, while the remaining information was confirmed in each person’s clinical process. From a total of 248 patients, only 116 met the eligibility criteria. A simple randomization was performed to select participants for both groups. Each group consisted of 35 patients. During the study, three patients withdrew, one from the intervention group due to a vacation period and two from the control group due to hospitalization. The study was concluded by 34 patients from the intervention group and 33 patients from the control group. Procedures Approval was obtained from the ethics committees of Diaverum (Approval No 1/2015). The patients were informed of the purpose of the study and of the right to withdraw without risk to oneself, plus, guaranteed data confidentiality. Those who met the inclusion criteria and agreed to participate gave informed consent. Privacy was guaranteed by curtains. A script was developed to support data collection and five nurses were trained to use it. Data collection was performed during the hemodialysis sessions. The intervention consisted in the visualization of humor movies during hemodialysis sessions. Each patient viewed the movie on their own monitor, using headphones to avoid distracting factors. The duration of the movie varied from patient to patient according to each one’s preference. The intervention program was applied for four weeks, two to three times a week, on Mondays, Wednesdays and Fridays. Between nine and ten interventions were undertaken. The movies portfolio was based on a previous study about the factors that influence the visualization of movies in patients undergoing hemodialysis9. Each movie lasted between 40 and 120 minutes. From the movies portfolio mentioned in the study9, the movies viewed during the session were selected according to each person’s preference. The control group viewed neutral movies such as documentaries and television programs during ten sessions over a four-week period. Data was collected using various tools, namely, a sociodemographic and health information questionnaire; the Subjective Happiness Scale (SHS)10-12; the satisfaction with life in general (SWLG) measured through the Personal Wellbeing Index (PWI)13-15; Depression Anxiety Stress Scale 21 (DASS-21)16-18, and Multidimensional Sense of Humor Scale (MSHS)19-21. Outcomes measurement The SHS is comprised of four items. In the second and third items, participants are asked to self-characterize themselves in comparison to their peers in both absolute and relative terms. Descriptions of happiness and unhappiness corresponded to items one and four. The score of the last item is reversed. The SHS requires the respondents to self-characterize using a visual analogue scale with seven positions. The scale is based on two antagonistic statements, expressing the level of happiness10-11. The Portuguese version applied to hemodialysis patients presents a single factor with an internal reliability with a Cronbach’s a of 0.9012. The SWLG consists of seven domains measuring life-satisfaction (satisfaction with the standard of living, health, personal development, personal relationships, sense of security, connection to the community, and security for the future). The respondents are asked to classify their satisfaction for each statement using a scale from 0 (extremely dissatisfied) to 10 (very satisfied). The SWLG is calculated using a scale from 0 to 100 (maximum percentage of the scale)13-14. The Portuguese version in hemodialysis patients revealed the existence of a single factor, with an internal reliability with a Cronbach’s a of 0.8215. DASS-21 provides a method for assessing and evaluating the effects of clinical intervention directed towards the communities who suffer emotional distress16-17,22. It is organized into three subscales: depression, anxiety and stress; each consisting of seven items16-17. The Portuguese version of DASS-21 in hemodialysis patients has a bidimensional structure, “Depression” and “Stress/Anxiety”, with alpha Cronbach values of 0.86 for “Depression” and 0.88 for “Stress / Anxiety”18. The MSHS presented an interpretable factor structure globally consistent with studies conducted with other samples, satisfactory internal consistency values. Therefore, the MSHS can be considered a valid instrument to characterize individuals regarding their “humorous state” and can describe sense of humor in its various dimensions19-20. A structure with three factors, “Humor Production and Social Use of Humor”, “Adaptive Humor and Appreciation Humor” and “Attitude Towards Humor”, with alpha Cronbach values of 0.93, 0.90 and 0.83 respectively, was revealed by the Portuguese version of MSHS21. Data analysis The scales and subscales scores,12,15,18,21 were calculated before (t1) and after intervention (t2). The normal distribution was verified by the KS test, since it is necessary to have large samples (n>30) to use the central limit theorem in order for student t-tests and t-tests for paired samples to be valid. Once asymmetry was found, the conclusions obtained were ‘confirmed’ using Mann Whitney U (two groups) and Wilcoxon (paired samples). The indexes and indicators of responsiveness most used to evaluate the response to change are: the percentage of change, ceiling effect and floor effect, effect size (ES), and the standardized response mean (SRM)23. ES and SRM are the most common parametric response measure A positive ES/SRM reflects improvement (normalized) in health or function in the standard deviation of the base score (for ES), or the difference in score between pre and post intervention values (for SRM). A ES> 0.80 is considered to have a large size effect; 0.50-0.79 a moderate effect, and ES <0.50 represents a small effect24. The ES and SRM calculation were performed using the MedCalc Version 15.8 software. The remaining statistical analyses were performed with the Statistical Package for Social Sciences (SPSS), version 20.3. Results When comparing the groups, some differences were found between the intervention sample and the control group. In the intervention group, 29.4% of the participants were of another nationality (from an African country), whereas in the control group these were only 6.1%. The educational level was also higher in the intervention group while 42.4% of the participants only had the 4th grade in the control group. Concerning marital status, in the intervention group 52.9% of the participants were married, whereas in the control group a higher percentage of participants was found (81.8%). With respect to gender, professional activity, presence of hypertension and diabetes mellitus, no differences were found between the intervention and the control group. Next, the results on the impact of the visualization of humor movies during the hemodialysis sessions, namely on subjective well-being, psychological health and sense of humor will be presented. In the beginning of the intervention there were no statistically significant differences in the means of the variables under study between both groups. The intervention group showed the highest percentages of change in stress and anxiety (-20.6%), depression (-43.2%) and attitude towards humor (9.8%). In the intervention group, the highest percentages of change occurred in the components: stress and anxiety (23.9%), humor production and social use of humor (-16.1%) and adaptive humor and appreciation humor (-13.1%) (Table 1). | |
| |
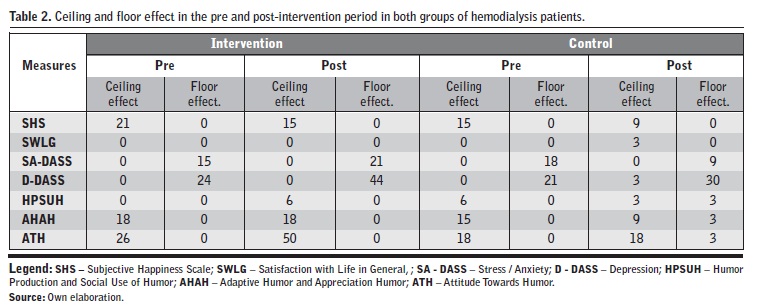
In the first evaluation, the intervention group presented a ceiling effect for subjective happiness in 21% of the cases, but it decreased to 15%, after the humor intervention. For stress and anxiety, the floor effect was 15% before the intervention and 21% after it. With regards to depression, the floor effect was 24% before the intervention and 44% in the post-intervention period (Table 2). | |
| |
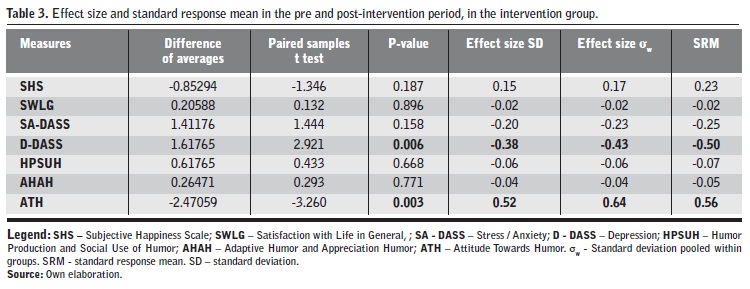
In humor production and social use of humor, during the pre-intervention period there was no ceiling effect, but after the intervention there was an increase of 6%. Regarding adaptive humor and appreciation humor, 18% of the sample presented a ceiling effect which was maintained after the intervention. On what concerns the attitude towards humor, the first evaluation revealed 26% of ceiling effect and after the intervention it rose to 50%. In the control group it was found that, in satisfaction with life in general, there was an increase of the ceiling effect from 0% to 3%. In stress and anxiety, the control group showed a decrease in the floor effect between evaluations from 18% to 9%, which translates into increased stress and anxiety in this group. Concerning depression, there was a 3% increase in the ceiling effect and an increase in the floor effect from 21% to 30%. In humor production and social use of humor there was a decrease in the ceiling effect from 6% to 3% and there was a 3% increase in the floor effect. In adaptive humor and appreciation humor there was a decrease in the ceiling effect from 15% to 9% and an increase in the floor effect of 3%. In the attitude towards humor there was no change in the ceiling effect (it remained at 18%), but there was an increase of 3% in the floor effect. In the intervention group it was found that the effects of size and standardized response mean were moderate and significant, in depression (negative) and in attitude towards humor (positive). There were small effects on stress / anxiety and negative affect, but they were not significant (Table 3). | |
| |
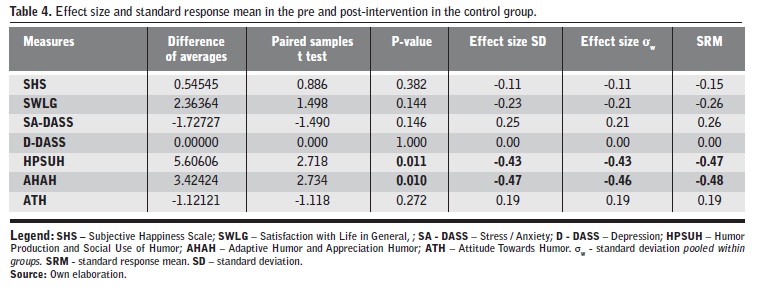
In the control group, moderate and negative ES and SRM were found to be negative and significant in the production of humor and social use of humor, and adaptive humor and appreciation humor. In the remaining variables it was also found moderate to low effects, but not significant, except for depression (Table 4). | |
| |
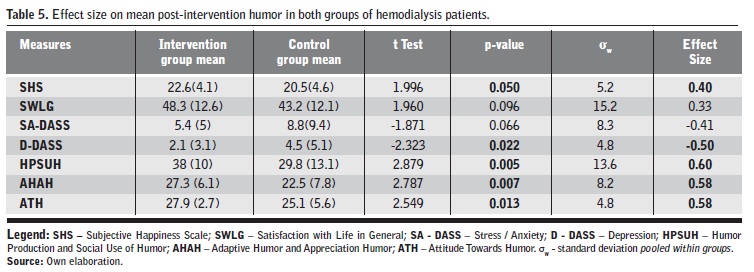
When comparing the intervention groups with the control group in the post-intervention period, there were significant moderate size effects on depression (negative), on the dimensions of the sense of humor (positive). There was a small to moderate size effect on happiness (positive). Moderate non-significant to moderate effects on life satisfaction (positive) and stress / anxiety (negative) were observed (Table 5). | |
| |
It was partially proved that watching humor movies during hemodialysis sessions improves subjective well-being in hemodialysis patients, that is, subjective happiness, satisfaction with life in general. The levels of subjective happiness increased in the intervention group, but there were no significant increases in satisfaction with life in general. It was also partially confirmed that watching humor movies during hemodialysis sessions decreased levels of stress / anxiety and depression in hemodialysis patients. Only depression levels decreased significantly in the intervention group. It is confirmed that watching humor movies during the hemodialysis sessions improves the sense of humor in hemodialysis patients. At the end of the intervention all sense of humor dimensions were improved in the group that viewed humor movies. Discussion In this research, in the intragroup analysis results (comparison before and after intervention), the intervention group had a decrease in depressive symptoms. A recent exploratory and descriptive study with a qualitative approach emphasizes that nurses play a preponderant role in patients with depression, being the most qualified in terms of caring, since all discourses present in the study point to positive ideas regarding the meaning of nurse. However, nurses report not having enough knowledge or time to properly approach these patients. This idea leaves no doubt about the importance of the development of scientific studies and training of professionals in this area25. The results are based on the findings of some experimental and quasi-experimental studies in the field of humor and humor therapy involving samples with elderly people26-27 and people with spinal cord injury28, which also showed a decrease in depressive symptoms. In the intragroup analysis, attitude towards humor improved in the intervention group after the visualization of humor movies over four weeks and there were no significant changes in the control group. Hence, it is important to integrate some activities of humor intervention (humor movie visualization) in nursing care in order to improve attitudes towards humor in hemodialysis patients. The intervention group showed significant differences in relation to the control group in subjective happiness, depression and the dimensions of the sense of humor. Despite not being statistically significant, it is also worth mentioning the existence of an increase in the satisfaction with life in general and in stress / anxiety. In this research, the levels of subjective happiness increased significantly. However, in a Bennett et al.6 study in hemodialysis patients, the increase was not statistically significant. Within simples with elderly people, humor increased the levels of happiness29-30 as well as, in subjective health and well-being, namely, satisfaction with life, general well-being23 and general health31. In this study, depression declined in the intervention group and the same occurred in studies involving older people26-27, however, in two other studies there were no changes in depression31-32. The levels of stress / anxiety decreased but were not significant, similarly to the study of laughter yoga in hemodialysis patients6. In studies with elderly people, anxiety levels26,31 and somatic symptoms31 decreased, but not stress31. Also, in this population there was a reduction of agitation29,32, insomnia27,31 and sleep quality improvement27. Sense of humor has a multidimensional character33-34. In this study, the three dimensions of sense of humor in hemodialysis patients improved in the intervention group when compared to the control group. However, factors that can influence sense of humor must be considered, namely, sex, age and disease situation33. Practical implications for nursing The improvement of the sense of humor dimensions can influence well-being, namely, increasing the level of subjective happiness, satisfaction with life in general, also decreasing depressive symptoms. All mood-based interventions are effective in improving depressive symptoms, with low-intensity effects immediately after the intervention35. Such data suggest a systematic intervention to effectively reduce depressive symptoms. The prescription of humor movies and comedies may be a therapeutic alternative to be implemented in patients during hemodialysis. Since people often use humor and laughter when they share their stories, nurses just need to improve their sense of humor for it to become a potential therapy, as this can be used to decrease pain, anxiety, stress, depression, and fatigue, and improve immunity, quality of life, joy, quality of sleep and resilience36. This study may contribute to the use of humor intervention in NANDA-International Nursing Diagnoses37, as well as, in the application of the nursing process supported by the International Classification for Nursing Practice (ICNP)38. We suggest the visualization of humor movies, particularly in patients diagnosed with deficit of recreation activities. Keeping in mind that humor intervention has, as mentioned before, the characteristics of a complex intervention, this research brought contributions to the prescription of the visualization of movies during hemodialysis sessions. It was possible to know which factors influence the initial evaluation, nurses must identify the factors that influence the appreciation of humor movies and the preferences of each person. During the humor intervention implementation, it is necessary to attend people’s choices, in order to individualize nursing care and deal with the paradoxical effect of humor34. Finally, the implications of this research on nurse education / training are related to the activities of humor intervention that may be prescribed in some nursing diagnoses referred to above. It is suggested the inclusion of humor intervention in the nursing curricula for undergraduate, post-graduate and specialization degrees. Limitations Although the samples were randomly selected in both groups, participants belonged to different clinics, which conditioned their allocation for a true experimental study. There may be factors that have not been controlled by belonging to different nursing teams and contexts and these variables can influence humor34. For future research it is recommended to use larger samples and the inclusion of a control group with the same characteristics, namely the context and health team, to examine the effects of humor during the sessions. It would also be an asset to evaluate the implementation of this intervention over a longer time span. According to the results obtained, it can be observed that the visualization of humor movies as a nursing intervention improves the levels of subjective happiness, and sense of humor, and decreases the perception of depressive symptoms. This study contributed to the understanding of humor effect on the psychological health, well-being and sense of humor in hemodialysis patients. The prescription of humor movies by nurses is a low intensity intervention that besides being a resource that allows to pass time during hemodialysis sessions, also has benefits in the health and quality of life of these people. Given the limitations and implications for practice identified in this study, we emphasize the need for further studies on nursing interventions in the field of sense of humor promotion in hemodialysis patients and its contribution to the well-being of this population.
Bibliografía 1. Costa FG, Coutinho MPL. Hemodiálise e depressão: representação social dos pacientes. Psicol Estud. 2014;19(4),657-67. doi:10.1590/1413-73722381608. 2. Moya Ruiz MA. Estudio del estado emocional de los pacientes en hemodiálisis. Enferm Nefrol. 2017 En-Mar;20(1):48-56. 3. Sousa LM, Antunes AV, Baixinho CR, Severino SS, Marques-Vieira C, José HM. Subjective Wellbeing Assessment in People with Chronic Kidney Disease Undergoing Hemodialysis. In: Rath T, editor. Chronic Kidney Disease: from Pathophysiology to Clinical Improvements. InTechOpen; 2018. p.281-93. 4. Mesa-Melgarejo L, Carrillo-Algarra AJ, Castiblanco RA, Reina LM, Ávila TM. Terapias de sustitución de la función renal: metaestudio y síntesis de evidencias cualitativas. Aquichan. 2017;17(3):328-52. 5. Sousa LM, Antunes AV, Marques-Vieira CM, Valentim OS, José HM. Qualidade de vida e pessoa com doença renal crónica: um estudo transversal. In: R Missias-Moreira, ZN Sales, LCG Nascimento, OS Valentim, editors. Qualidade de vida e condições de saúde de diversas populações. Curitiba: Editora CRV; 2017(2):139-54. 6. Bennett PN, Parsons T, Ben-Moshe R, Neal M, Weinberg MK, Gilbert K, et al. Intradialytic Laughter Yoga therapy for haemodialysis patients: a pre-post intervention feasibility study. BMC Complement AlternMed. 2015 Jun 9; 15:176-82. 7. Mehrabi Y, Ghazavi Z, Shahgholian N. Effect of fordyce’s happiness program on stress, anxiety, and depression among the patients undergoing hemodialysis. Iran J Nurs Midwifery Res. 2017 May-Jun; 22(3):190-4. 8. Martin RA. Humor, laughter, and physical health: methodological issues and research findings. Psychol Bull. 2001 Jul;127(4):504-19. doi:10.1037/0033-2909.127.4.504. 9. Sousa LM, Marques-Veira C, Severino SS, Pozo-Rosado JL, José HM. Fatores explicativos da apreciação de filmes cómicos em pessoas com doença renal crónica. Rev Inv Enferm. 2016 Apr; (15):49-55. 10. Lyubomirsky S, Lepper HS. A measure of subjective happiness: Preliminary reliability and construct validation. Soc Ind Res. 1999 Feb 1;46(2):137-55. doi: 10.1023/A:1006824100041. 11. Pais-Ribeiro JL. Validação transcultural da Escala de Felicidade Subjectiva de Lyubomirsky e Lepper. Psicol Saúde Doenças [Internet]. 2012 [cited 2018 Sep 10]; 13 (2): 157-168. Available from: http://www.scielo.mec.pt/scielo.php?pid=S1645-00862012000200003&script=sci_arttext&tlng=es. 12. Sousa LM, Vieira CM, Severino SS, Pozo-Rosado JL, José HM. Validation of the Subjective Happiness Scale in people with Chronic Kidney Disease. Enferm Global. 2017 Jul; 16 (3):60-70.: doi:10.6018/eglobal.16.3.266571. 13. Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singap. 1994 Mar [cited 2018 Sep 10];23(2):129-38. Available from: https://psycnet.apa.org/record/2015-49222-001. 14. Ferreira-Valente MA, Pais Ribeiro JL, Jensen MP. Contribución adicional para la validación de la versión portuguesa de la Escala de Interferencia del Inventario Breve de Dolor. Clín Salud. 2012 Mar [cited 2018 Sep 10];23(1):89-96. Available from: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1130-52742012000100005. 15. Sousa LMM, Marques-Vieira CMA, Severino SSP, Pozo Rosado JL, José, MHG. Validación del Índice de Bien-estar Personal en personas con enfermedad renal crónica. Enferm Nefrol. 2016 Jun; 19(2):135-41. doi:10.4321/S2254-28842016000200005. 16. Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995 Mar 1;33(3):335-43. doi:10.1016/0005-7967(94)00075-U. 17. Pais-Ribeiro JL, Honrado A, Leal I. Contribuição para o estudo da adaptação portuguesa das escalas de ansiedade, depressão e stress (EADS) de 21 itens de Lovibond e Lovibond. Psicol Saúde Doenças. 2004 Nov [cited 2018 Sep 10];5(2):229-39. Available from: http://www.scielo.mec.pt/scielo.php?pid=S1645-00862004000200007&script=sci_arttext&tlng=en. 18. Sousa LM, Marques-Vieira CM, Severino SS, Pozo-Rosado JL, Gomes JC, José HM. A Depression Anxiety Stress Scale em pessoas com doença renal crónica. Rev Port Enferm Saude Ment. 2017 Jun; 17:50-7.: doi:10.19131/rpesm.0182. 19. Thorson JA, Powell FC. Development and validation of a multidimensional sense of humor scale. J Clinic Psychol. 1993 Jan;49(1):13-23. doi:10.1002/1097-4679(199301)49:1<13::AID-JCLP2270490103>3.0.CO;2-S. 20. José H, Parreira P. Adaptação para Português da Escala Multidimensional do Sentido de Humor MSHS. Referência.[Internet]. 2008 [cited 2018 Sep 10];6:7-18. Available from: http://hdl.handle.net/10400.14/7524. 21. Sousa LMM, Marques-Vieira CM, Severino S, Pozo-Rosado J, Antunes AV, José H. Validation of the multidimensional sense of humor scale in people with chronic kidney disease. J Nurs Educ Pract. 2018; 8(3):72-9. doi:10.5430/jnep.v8n3p72. 22. Moussa MT, Lovibond P, Laube R, Megahead HA. Psychometric properties of an arabic version of the depression anxiety stress scales (DASS). Res Soc Work Pract. 2017 May;27(3):375-86. doi:10.1177/1049731516662916. 23. Sousa LM, Marques-Vieira C, Severino S, Caldeira S. Propriedades psicométricas de instrumentos de avaliação para a investigação e prática dos enfermeiros de reabilitação. In C. Marques-Vieira, L. Sousa (Eds). Cuidados de Enfermagem de Reabilitação à Pessoa ao Longo da Vida. Loures: Lusodidacta. 2017:113-122. 24. Angst F, Goldhahn J, Drerup S, Kolling C, Aeschlimann A, Simmen BR, S et al. Responsiveness of five outcome measurement instruments in total elbow arthroplasty. Arthritis Care Res. 2012 Nov;64(11):1749-55. 25. Guedes CR, Alvarenga BD, Rotella I, Vilella DV. Habilidades do Enfermeiro no Diagnóstico e Cuidado ao Portador de Depressão/Nursing Skills in Diagnosis and Care For Patients With Depression. Rev Ciênc Saúde. 2015;5(4):13-9. doi:10.21876/rcsfmit.v5i4.402. 26. Ganz FD, Jacobs JM. The effect of humor on elder mental and physical health. Geriatr Nurs. 2014 May; 35(3):205-11. 27. Ko HJ, Youn CH. Effects of laughter therapy on depression, cognition and sleep among the community dwelling elderly. Geriatr Gerontol Int. 2011 Jul;11(3):267-74. 28. Beh-Pajooh A, Jahangiri M, Zahrakar K. Humor skills training and reducing depression in patients with spinal cord injury. J Iran Psychol. 2010; 6(1):227-36. 29. Low LF, Goodenough B, Fletcher J, Xu K, Casey AN, Chenoweth L, et al. The effects of humor therapy on nursing home residents measured using observational methods: The SMILE cluster randomized trial. J Am Med Dir Assoc. 2014; 15(8):564-9. 30. Tse MM, Lo AP, Cheng TL, Chan EK, Chan AH, Chung HS. Humor Therapy: Relieving Chronic Pain and Enhancing Happiness for Older Adults. J Aging Res. 2010;33:1-9. 31. Ghodsbin F, Jahanbin I, Sharif F. The effects of laughter therapy on general health of elderly people referring to jahandidegan community center in shiraz, iran, 2014: a randomized controlled trial. Int J community based Nurs midwifery. 2015 Jan; 3(1):31-8. 32. Low LF, Brodaty H, Goodenough B, Spitzer P, Bell JP, Fleming R, et al. The Sydney Multisite Intervention of LaughterBosses and ElderClowns (SMILE) study: cluster randomised trial of humour therapy in nursing homes. BMJ open. 2013 Jan; 1;3(1):e002072. 33. José H, Parreira P. Adaptação para Português da Escala Multidimensional do Sentido de Humor MSHS. Referência. 2008;SII(6):7-18. 34. Sousa LM, José HM. Benefícios do humor na saúde Revisão Sistemática da Literatura. Enformação. 2016;7:22-32. 35. Wellenzohn S, Proyer RT, Ruch W. Humor-based online positive psychology interventions: a randomized placebo-controlled long-term trial. J Posit Psychol. 2016 Nov;11(6):584-94. doi:10.1080/17439760.2015.1137624. 36. Bennett PN, Parsons T, Ben-Moshe R, Weinberg M, Neal M, Gilbert K, et al. Laughter and humor therapy in dialysis. Sem Dial. 2014 Sep;27(5):488-93. 37. Herdman HT, Kamitsuru S, (eds). Nursing Diagnoses: Definitions & Classification 2018-2020. 11th ed. Stuttgart: Thieme; 2017:184-383. 38. International Council of Nurse. International Classification for Nursing Practice (ICNP®). Geneva: International Council of Nurse; 2015. Este artículo se distribuye bajo una Licencia Creative Commons Atribución-NoComercial 4.0 Internacional.
| |
|